AUCTORES
Globalize your Research

Review | DOI: https://doi.org/10.31579/2693-4779/056
North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, Manchester, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo. North Manchester General Hospital, Department of Urology, Delaunays Road, Crumpsall, Manchester, United Kingdom.
Citation: Anthony K-G Venyo. (2021) Coronavirus Infection of the Urinary Bladder and Lower Urinary Tract: A Review and Update. Clinical Research and Clinical Trials. 4(2); DOI: 10.31579/2693-4779/056
Copyright: © 2021 Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 July 2021 | Accepted: 09 August 2021 | Published: 18 August 2021
Keywords: coronavirus; covid-19 infection; urinary bladder; lower urinary tract symptoms; urinary frequency; urgency; incontinence; retention of urine; haematuria; isolation
COVID-19 infection does affect males and females. Even though the commonest manifestations of COVID-19 infection tend to be related to symptoms associated with the respiratory tract, many other organs of the body also tend to be affected and COVID-19 infection of these other organs could manifest contemporaneously with symptoms of the respiratory tract system in addition to symptoms of the affected organs. At times COVID-19 may initially manifest solely related to non-respiratory tract organs and because the symptoms are non-specific without a high index of suspicion, the diagnosis of COVID-19 infection may be missed initially or there may be delay in the diagnosis which would tend to lead to spreading of the disease. Some of the manifestations of COVID-19 infection of the urinary bladder may include: Lower urinary tract symptoms of urinary frequency, and or urinary urgency, and or nocturia, and or urinary incontinence, or on rare occasions non-visible or visible haematuria, or acute retention of urine. The aforementioned symptoms may occur as De novo (new-onset) symptoms alone or they may be associated with or without fever, with or without respiratory tract symptoms. Some individuals who already have lower urinary tract symptoms could experience worsening of their previous lower urinary tract symptoms and if the clinician does not have a high index of suspicion for the possible development of COVID-19 infection, and the clinician does blame the symptoms on benign prostatic hyperplasia then the diagnosis could be missed or delayed. If the COVID-19 cystitis is associated with COVID-19 infection of the male genital tract then some of the patients could experience scrotal discomfort, swelling of the scrotum, erythema of the scrotum, or low-flow priapism or clinical and radiology imaging features of acute orchitis, or acute epididymitis, or acute epididymo-orchitis. However, if the lower urinary tract symptoms are associated with respiratory tract symptoms all clinicians globally are aware of the fact that a high index of suspicion for COVID-19 infection should be exercised. What is important is that every clinician and every individual should be made aware of the fact that the development of De novo lower urinary tract symptoms or sudden onset of worsening lower urinary tract symptoms should be regarded as possibly due to COVID-19 infection and appropriate tests should be undertaken to confirm or negate the diagnosis of COVID-19 infection quickly. Diagnosis of COVID-19 infection of the urinary bladder can be confirmed the undertaking of various COVID-19 infection tests but COVID-19 PCR test has tended to be a common test that most people use globally.
The emergence of the COVID-19 pandemic has become a sudden global problem that has affected the entire world and all the Governments throughout the entire world in collaboration with the World Health Organization are making efforts to diagnose COVID-19 infection as well as to undertake mass vaccinations of individuals as an effort to prevent further spread of the disease. Even though COVID-19 infection most often manifests with non-specific respiratory tract symptoms, COVID-19 which can affect many organs of the body may also manifest with lower urinary tract symptoms for which clinicians and the public need to be aware of in order to have a high index of suspicion to exclude COVID-19 infections when patients present with sudden onset of urinary tract symptoms. Manifestations of COVID-19 infections have ranged from those of individuals who have asymptomatic manifestations to severe illnesses that tend to be ensued by death of the patients [1]. Some of the common manifestations of COVID-19 infection have included fever, cough, as well as shortness of breath [1, 2]. Other manifestations of COVID-19 infection that had been documented include malaise and respiratory distress [1, 3].
It has been iterated that symptoms that are associated with COVID-19 could develop 2 days to 2 weeks pursuant to exposure to the COVID-19 virus [1, 2]. It has also been documented that a pooled analysis of 181 confirmed cases of COVID-19 infection outside Wuhan in China had found that the mean incubation period of COVID-19 infection was 5.1 days as well as that 97.5% of individuals who had manifested with symptoms had done so within 11.5 days of the infection [1, 4].
Aboubaker et al. [5] made the ensuing summations related to COVID-19 infections:
The novel coronavirus (SARS-COV2) had led to an outbreak of many cases of pneumonia within the city of Wuhan in China in December 2019.
The disease which caused by this virus was given a terminology of Coronavirus disease 2019 or COVID-19, which had been declared by the World Health Organization (WHO) as a global pandemic in March 2020.
COVID-19 infection typically does manifest with respiratory tract symptoms as well as febrile illness. Nevertheless, there are a few reported cases of extra-pulmonary and atypical manifestations of COVID-19 infection including: haemoptysis, cardiac symptoms, neurological symptoms, gastrointestinal symptoms, ocular symptoms, cutaneous symptoms, venous and or arterial thrombosis.
Lack of awareness of the aforementioned manifestations of COVID-19 infection could led to: misdiagnosis of the disease, delay in the diagnosis of the disease, and delay in the isolation of suspected patients with COVID-19 infection which does increase the risk of transmission of COVID-19 infection between patients and doctors.
Altschul et al. [6] undertook a retrospective study that included a cohort of patients who had been admitted into one of three major hospitals within their network between 1st March 2020 and 1st May 2020. All of the patients had had undergone radiology imaging of their neuro-axis as well as they had positive PCR testing results for COVID-19 were identified and they were reviewed by an attending neuro-radiologist. The demographics as well as their co-morbidities were recorded. The results of the biomarkers were also recorded from the day of the haemorrhage event. The vital signs from the day of the haemorrhage event mechanical ventilation orders at admission were also recorded. The radiology imaging findings were sub-divided into 5 sub-types that included: acute subdural haematoma (SDH), subarachnoid haemorrhage (SAH), multi-compartmental haemorrhage (MCH), multi-focal-intracerebral haemorrhage (MFH), and a focal intracerebral haemorrhage (fICH). The outcomes were documented as non-routine discharge and mortality. Altchul et al. [6] summarized the results as follows:
They had found a total of 35 patients out of 5227 patients who had COVID-19 infection who had haemorrhage of some kind. Seventeen patients had presented with subdural haematoma (SDH), 2 patients had subarachnoid haemorrhage (SAH), 7 patients had multi-compartmental haemorrhage (MCH), 4 patients had multifocal-intracerebral haemorrhage (MFH), 5 patients had focal intracerebral haemorrhage (fICH).
Sixty eight point 6 percent (68.6%) of all of these patients had manifested with primary neurological symptoms within the emergency room.
Thirty one point 4 percent (31.4%) of the patients had acquired the aforementioned conditions as inpatients.
Thirty one point four percent (31.4%) of the patients also manifested with severe pulmonary COVID-19 symptoms that required mechanical ventilation upon admission.
Most of the patients did have concomitant intra-cerebral haemorrhage of some kind. (MCH = 85.7 %, MFH = 75 %, fICH = 40 %).
None of the patients who had subdural haematoma or subarachnoid haematoma had severe pulmonary COVID during their initial presentation.
Only 4 of the patients that amounted to 11.4% of the cases did undergo surgical treatment.
The mortality for the entire cohort of the patients amounted to 45.7% which accounted for 16 of the patients out of the 35 patients.
Patients who had SDH did have a mortality rate of 35.3% that amounted to 6 patients out of 17 patients.
Patients who had SAH had a mortality of 50 % that amounted to one patient out of two patients.
MCH patients had a mortality of 71.4 % that amounted to 5 patients out of 7 patients.
Patients who had MFH had a mortality of 50 % that amounted to 2 out of 4 patients.
Patients who had fICH patients had a mortality of 40 % that amounted to 2 out of 5 patients.
In comparison with patients who were discharged, the patients who died were mostly represented by Hispanics (56.3%), they had higher rates of severe COVID-19 infection upon admission (10.5% versus 56.3%, p = 0.004), higher rates of congestive cardiac failure (5.3% versus 31.3%, p = 0.042), higher rates of prolonged PTT > 38.9 s (0% versus 46.2%, p = 0.002), higher rates of INR > 1.2 (12.5% versus 61.5%, p = 0.006), mostly spontaneous haemorrhages (47.4% versus 81.3%, p = 0.039) as well as lower rates history of utilization of anti-platelet (26.3% versus 0%, p = 0.027).
Significant variables with regard to the univariate analysis plus variables with P <0> 40 U/L, and AST > 40 U /L had been included in the multivariate logistic regression, patients who had severe pulmonary COVID-19 that required mechanical ventilation (OR 10.24 [43-243.12] p = 0.015] p = 0.015), with INR > 1.2 on the day of the haemorrhagic event (OR 14.36) [1.69 – 122.14] p = 0.015], and patients who presented with spontaneous versus traumatic haemorrhage (OR 6.11 [31-118.89] p = 0.023) did have significantly higher risk of mortality.
Altschul et al. [6] made the following conclusions:
Haemorrhagic manifestations with COVID-19 infection are uncommon but serious way in which the COVID-19 illness can present.
It is important for neurosurgeons to appreciate that patients can manifest with the aforementioned findings without primary pulmonary symptoms, as well as that severe pulmonary symptoms do negatively affect the outcomes of the disease.
Green et al [7]. iterated the ensuing regarding the diagnostic tests that could be undertaken to confirm or establish the diagnosis of COVID-19 infection.
Various tests for the diagnosis of coronavirus disease (19) have been available so far and more tests for the diagnosis of COVID-19 infection are gaining emergency approval on daily basis.
These COVID-19 diagnostic tests tend to be mainly based upon four different techniques.
Firstly, the reverse transcription polymerase chain reaction (RT-PCR) test is the current standard test for the diagnosis of COVID-19 infection.
Secondly, loop-mediated isothermal amplification (LAMP) does represent a simple, but less developed for testing for COVID-19 infection.
Thirdly lateral flow tests represent a hand-held single use assays that do provide the results for an individual patient in as short as 15 minutes.
And fourthly Enzyme-linked immunosorbent assay (ELISA) which is a quick as well as technically simple assays that tend to be easily read and which offer relatively high throughput.
Millions of individuals who have COVID-19 infection do tend to present with respiratory tract symptoms which is well known by clinicians and patients throughout the world. Urinary tract symptom manifestations of patients who have COVID-19 infections are uncommon and in view of this it would be envisaged that globally majority clinicians including urologist would not be familiar with the urological manifestations of COVID-19 infection and when they see patients with COVID-19 infection that present with lower urinary tract symptoms they would most likely not have a high index of suspicion for COVID-19 infection which therefore tend to lead either to mis-diagnosis of the disease or delay in the correct diagnosis of the disease. The ensuing article on Corona Virus Infection of the Urinary Bladder; A Review and Update is divided into two parts: (A) Overview and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, and Studies Related to COVID-19 Infection of the Urinary Bladder.
The emergence of the COVID-19 pandemic has become a sudden global problem that has affected the entire world and all the Governments throughout the entire world in collaboration with the World Health Organization are making efforts to diagnose COVID-19 infection as well as to undertake mass vaccinations of individuals as an effort to prevent further spread of the disease. Even though COVID-19 infection most often manifests with non-specific respiratory tract symptoms, COVID-19 which can affect many organs of the body may also manifest with lower urinary tract symptoms for which clinicians and the public need to be aware of in order to have a high index of suspicion to exclude COVID-19 infections when patients present with sudden onset of urinary tract symptoms. Manifestations of COVID-19 infections have ranged from those of individuals who have asymptomatic manifestations to severe illnesses that tend to be ensued by death of the patients [1]. Some of the common manifestations of COVID-19 infection have included fever, cough, as well as shortness of breath [1, 2]. Other manifestations of COVID-19 infection that had been documented include malaise and respiratory distress [1, 3].
It has been iterated that symptoms that are associated with COVID-19 could develop 2 days to 2 weeks pursuant to exposure to the COVID-19 virus [1, 2]. It has also been documented that a pooled analysis of 181 confirmed cases of COVID-19 infection outside Wuhan in China had found that the mean incubation period of COVID-19 infection was 5.1 days as well as that 97.5% of individuals who had manifested with symptoms had done so within 11.5 days of the infection [1, 4].
Aboubaker et al. [5] made the ensuing summations related to COVID-19 infections:
The novel coronavirus (SARS-COV2) had led to an outbreak of many cases of pneumonia within the city of Wuhan in China in December 2019.
The disease which caused by this virus was given a terminology of Coronavirus disease 2019 or COVID-19, which had been declared by the World Health Organization (WHO) as a global pandemic in March 2020.
COVID-19 infection typically does manifest with respiratory tract symptoms as well as febrile illness. Nevertheless, there are a few reported cases of extra-pulmonary and atypical manifestations of COVID-19 infection including: haemoptysis, cardiac symptoms, neurological symptoms, gastrointestinal symptoms, ocular symptoms, cutaneous symptoms, venous and or arterial thrombosis.
Lack of awareness of the aforementioned manifestations of COVID-19 infection could led to: misdiagnosis of the disease, delay in the diagnosis of the disease, and delay in the isolation of suspected patients with COVID-19 infection which does increase the risk of transmission of COVID-19 infection between patients and doctors.
Altschul et al. [6] undertook a retrospective study that included a cohort of patients who had been admitted into one of three major hospitals within their network between 1st March 2020 and 1st May 2020. All of the patients had had undergone radiology imaging of their neuro-axis as well as they had positive PCR testing results for COVID-19 were identified and they were reviewed by an attending neuro-radiologist. The demographics as well as their co-morbidities were recorded. The results of the biomarkers were also recorded from the day of the haemorrhage event. The vital signs from the day of the haemorrhage event mechanical ventilation orders at admission were also recorded. The radiology imaging findings were sub-divided into 5 sub-types that included: acute subdural haematoma (SDH), subarachnoid haemorrhage (SAH), multi-compartmental haemorrhage (MCH), multi-focal-intracerebral haemorrhage (MFH), and a focal intracerebral haemorrhage (fICH). The outcomes were documented as non-routine discharge and mortality. Altchul et al. [6] summarized the results as follows:
They had found a total of 35 patients out of 5227 patients who had COVID-19 infection who had haemorrhage of some kind. Seventeen patients had presented with subdural haematoma (SDH), 2 patients had subarachnoid haemorrhage (SAH), 7 patients had multi-compartmental haemorrhage (MCH), 4 patients had multifocal-intracerebral haemorrhage (MFH), 5 patients had focal intracerebral haemorrhage (fICH).
Sixty eight point 6 percent (68.6%) of all of these patients had manifested with primary neurological symptoms within the emergency room.
Thirty one point 4 percent (31.4%) of the patients had acquired the aforementioned conditions as inpatients.
Thirty one point four percent (31.4%) of the patients also manifested with severe pulmonary COVID-19 symptoms that required mechanical ventilation upon admission.
Most of the patients did have concomitant intra-cerebral haemorrhage of some kind. (MCH = 85.7 %, MFH = 75 %, fICH = 40 %).
None of the patients who had subdural haematoma or subarachnoid haematoma had severe pulmonary COVID during their initial presentation.
Only 4 of the patients that amounted to 11.4% of the cases did undergo surgical treatment.
The mortality for the entire cohort of the patients amounted to 45.7% which accounted for 16 of the patients out of the 35 patients.
Patients who had SDH did have a mortality rate of 35.3% that amounted to 6 patients out of 17 patients.
Patients who had SAH had a mortality of 50 % that amounted to one patient out of two patients.
MCH patients had a mortality of 71.4 % that amounted to 5 patients out of 7 patients.
Patients who had MFH had a mortality of 50 % that amounted to 2 out of 4 patients.
Patients who had fICH patients had a mortality of 40 % that amounted to 2 out of 5 patients.
In comparison with patients who were discharged, the patients who died were mostly represented by Hispanics (56.3%), they had higher rates of severe COVID-19 infection upon admission (10.5% versus 56.3%, p = 0.004), higher rates of congestive cardiac failure (5.3% versus 31.3%, p = 0.042), higher rates of prolonged PTT > 38.9 s (0% versus 46.2%, p = 0.002), higher rates of INR > 1.2 (12.5% versus 61.5%, p = 0.006), mostly spontaneous haemorrhages (47.4% versus 81.3%, p = 0.039) as well as lower rates history of utilization of anti-platelet (26.3% versus 0%, p = 0.027).
Significant variables with regard to the univariate analysis plus variables with P <0> 40 U/L, and AST > 40 U /L had been included in the multivariate logistic regression, patients who had severe pulmonary COVID-19 that required mechanical ventilation (OR 10.24 [43-243.12] p = 0.015] p = 0.015), with INR > 1.2 on the day of the haemorrhagic event (OR 14.36) [1.69 – 122.14] p = 0.015], and patients who presented with spontaneous versus traumatic haemorrhage (OR 6.11 [31-118.89] p = 0.023) did have significantly higher risk of mortality.
Altschul et al. [6] made the following conclusions:
Haemorrhagic manifestations with COVID-19 infection are uncommon but serious way in which the COVID-19 illness can present.
It is important for neurosurgeons to appreciate that patients can manifest with the aforementioned findings without primary pulmonary symptoms, as well as that severe pulmonary symptoms do negatively affect the outcomes of the disease.
Green et al [7]. iterated the ensuing regarding the diagnostic tests that could be undertaken to confirm or establish the diagnosis of COVID-19 infection.
Various tests for the diagnosis of coronavirus disease (19) have been available so far and more tests for the diagnosis of COVID-19 infection are gaining emergency approval on daily basis.
These COVID-19 diagnostic tests tend to be mainly based upon four different techniques.
Firstly, the reverse transcription polymerase chain reaction (RT-PCR) test is the current standard test for the diagnosis of COVID-19 infection.
Secondly, loop-mediated isothermal amplification (LAMP) does represent a simple, but less developed for testing for COVID-19 infection.
Thirdly lateral flow tests represent a hand-held single use assays that do provide the results for an individual patient in as short as 15 minutes.
And fourthly Enzyme-linked immunosorbent assay (ELISA) which is a quick as well as technically simple assays that tend to be easily read and which offer relatively high throughput.
Millions of individuals who have COVID-19 infection do tend to present with respiratory tract symptoms which is well known by clinicians and patients throughout the world. Urinary tract symptom manifestations of patients who have COVID-19 infections are uncommon and in view of this it would be envisaged that globally majority clinicians including urologist would not be familiar with the urological manifestations of COVID-19 infection and when they see patients with COVID-19 infection that present with lower urinary tract symptoms they would most likely not have a high index of suspicion for COVID-19 infection which therefore tend to lead either to mis-diagnosis of the disease or delay in the correct diagnosis of the disease. The ensuing article on Corona Virus Infection of the Urinary Bladder; A Review and Update is divided into two parts: (A) Overview and (B) Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, and Studies Related to COVID-19 Infection of the Urinary Bladder.
To review and update the literature on Corona Virus (COVID-19) Infection of the Urinary Bladder.
Internet data bases were searched including google, google scholar, yahoo, and PUBMED. The search words that were used included Corona virus infection of bladder; COVID-19 cystitis; COVID-19 Lower Urinary Tract Symptoms; Covid-19 Urinary Tract Symptoms. Coronavirus bladder infection. Forty four references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed some general aspects of Coronavirus infection, and (B) Miscellaneous narrations and discussions related to Coronavirus (COVID-19) infection case reports, case series as well as some studies related to Coronavirus infections of the urinary bladder.
Results Review and Update of Literature on Coronavirus (COVID-19) Infection of the urinary bladder as Well as Lower Urinary Tract Symptoms.
Overview
Definition / General Statements
Coronavirus disease 2019 is stated to be a disease which is caused by a single stranded ribonucleic acid (RNA) virus which does belong to the genus Beta Coronavirus [8].
The terminology that has been coined for the causative agent for coronavirus disease / infection is SARS-Co-2 which refers to severe acute respiratory syndrome coronavirus 2 in view of its similarities to the virus which had caused the SARS epidemic in the year 2003 [8, 9].
Public health emergency related to Coronavirus disease 2019 (COVID-19) was declared by the United States of America Secretary of Health and Human Services on the 31st of January 2020 [8,10]
It has been iterated that Corona Virus (COVID – 19) pandemic was declared by the World Health Organization (WHO) on the 11th of March 2020 [8].
It has additionally been iterated that the Genome of COVID-19 is likely that of the genome of bat origin [8,11].
Clinical Manifestations
Symptoms of COVID-19 infection are said to be most often mild to moderate but the symptoms could be severe or fatal, especially among the elderly and those patients who have underlying illnesses [8]
Typical signs and symptoms of COVID-19 infection tend to include: fever, cough and dyspnoea [8]
Other symptoms of COVID-19 infection do include chills, muscle pain, sore throat as well as loss of taste or smell
It has been documented that the Incubation period of COVID-19 infection has tended to range between: 2 days and - 14 days [8,12]
It has been stated that children of all ages are at risk for the development of COVID-19 infection but complications of COIVID-19 infection generally appear to be less common in comparison with adults[8,13]
Symptoms of COVID-19 could simulate those of common viral respiratory tract infections, which would require appropriate suspicion for COVID-19 infection as well as consideration for other infectious aetiologies
A serious multi-system inflammatory syndrome in children (MIS-C) has been reported up to 21 years of age
Covid-19 infection could manifest with fever, raised levels of serum inflammatory markers and multi-organ involvement, including rash, abdominal pain and myocarditis [8,14]
COVID-19 infection does bear similarities with toxic shock syndrome and Kawasaki disease including:
Febrile illness that is characterized by vasculitis
Presenting as rash, skin peeling, cervical lymph node enlargements, swelling of the hands and feet as well as gastrointestinal symptoms [8]
Elevated levels of interleukin 6 (median 135 pg/mL) and d-dimer (median 5284 ng/mL) in one cohort of 35 MIS-C patients [15]
MIS-C could begin weeks pursuant to infection with SARS-CoV-2 [8] pathologyoutlines.com]
Essential features of laboratory testing
It was iterated that the emergency use authorization (EUA), had put into place by United States of America (USA) Congress, which allows for expedited Food and Drug Administration (FDA) review within 24 hours in many cases of COVID-19 infection based upon less stringent validation standards than in nonurgent situations [8,16]
Emergency use authorization adoption had led to rapid expansion of testing capacity in the United .S. since middle of March, 2020 [8]
Increasing demand continues to outpace assay reagents and supplies [8]
FDA has provided further flexibility by allowing commercial launch of a diagnostic assay as early as 15 business days prior to emergency use authorization submission as of March 1, 2020 [8,17]
Samples in a laboratory should be handled in a class II or higher biological safety cabinet [8,18]
Testing priorities
Guidelines for patient testing established by the U.S. Centers for Disease Control (CDC) [8]
Previously considered “nonpriority”, some asymptomatic individuals are now considered “priority” for testing due to the possibility of asymptomatic infection and viral shedding that can lead to disease transmission [8]
Guidance updated on May 3, 2020 to test certain asymptomatic individuals as a part of public health surveillance or a mitigation strategy in long term care facilities and other settings [8,19]
Broader testing guidelines reflect the need for more aggressive infection control measures as well as the increased availability of commercial assays, reagents and supplies [8]
High priority: [8]
Hospitalized patients with symptoms
Healthcare facility workers, workers in congregate living settings and first responders with symptoms
Residents in long term care facilities or other congregate living settings, including prisons and shelters, with symptoms
Priority: [8]
Persons with symptoms of potential COVID-19 infection including fever, cough, shortness of breath, chills, muscle pain, new loss of taste or smell, vomiting or diarrhoea or sore throat
Persons without symptoms who are prioritized by health departments or clinicians, for any reason, including but not limited to public health monitoring, sentinel surveillance or screening of other asymptomatic individuals according to state and local plans
Special considerations for healthcare personnel: [8]
Testing may be considered if there has been exposure to a person with suspected (not yet confirmed) COVID-19
Even mild signs and symptoms (e.g., sore throat) of COVID-19 should be evaluated in healthcare personnel who may be potentially exposed, in order to protect vulnerable patients they may come in contact with
Special considerations for children and young adults with MIS-C [8]
May represent a post-viral syndrome or cytokine storm caused by body’s immune response
Incubation period may be up to 4 weeks (longer than that seen in adults with respiratory symptoms)
Serology testing more likely positive than RT-PCR for SARS-CoV-2 in one small cohort of 10 Italian children [8,20]
Special considerations for neonates [8,21]
Testing recommended for all neonates born to mothers with confirmed or suspected COVID-19, whether or not there are any signs and symptoms in the neonate or the mother
RNA testing by RT-PCR on nasopharyngeal, oropharyngeal or nasal swab samples
Evolution of diagnostic testing [8]
CDC was the first in the U.S. to develop a SARS-CoV-2 diagnostic assay
Emergency use authorization received on February 4, 2020
Real time reverse transcriptase polymerase chain reaction (rRT-PCR)
Gene target: SARS-CoV-2 nucleocapsid (N) gene [22]
Platform: Applied Biosystems 7500 Fast DX Real Time PCR System [23]
Encountered manufacturing issues with a failed reagent released to public health laboratories, which limited availability of testing outside the CDC [24]
New York state department of public health developed its own molecular assay to satisfy unmet demands; granted second emergency use authorization on February 29, 2020 [8,25].
Virus samples became available to private assay developers for validation in late February, 2020 [8]
Rapidly growing list of commercial assays since mid-March, 2020 (exceeding 25 as of April 10, 2020) [8,26]
Technology platforms [8]
Current commercial in vitro diagnostic assays typically feature:
Qualitative rRT-PCR for amplification of viral RNA in respiratory samples
Dual or triple amplification targets may include genetic sequences from nucleocapsid (N) gene, envelope (E) gene, spike (S) protein or ORF1ab
First commercial molecular assay to receive emergency use authorization: Roche cobas (March 12, 2020)
Rapid point of care assay by Abbott Diagnostics granted emergency use authorization on March 27, 2020 based on isothermal nucleic acid amplification
Serology assay, typically either a rapid diagnostic test (lateral flow assay) or enzyme linked immunoassay (ELISA) to detect IgM and IgG antibody immune response in the blood
May be helpful for retesting symptomatic / suspected patients who have tested negative by molecular method
Can help to determine who has immunity and who may donate convalescent plasma in the proper clinical context [8,27]
May help to identify asymptomatic infection as a part of contact tracing or mitigation strategy [8]
Seroconversion of 50% at 13 days (median) and 100% at 19 days after symptom onset in 1 cohort of 285 patients. [8,28]
Not for sole diagnosis of acute illness [8]
FDA review waived for serology assays as of March 16, 2020, upon assay validation, notification of the FDA and inclusion of a disclaimer [8,27]
First serology assay received emergency use authorization on April 1, 2020, by Cellex for testing serum, plasma or whole blood from venipuncture in the laboratory [8,29]
Many are being developed or released in the U.S., some of which have been in use in other countries
First next generation sequencing (NGS) assay under COVID-19 EUA (6/9/2020): Illumina COVIDSeq Test [8]
High throughput sequencing of amplified viral RNA
Detects 98 targets on SARS-CoV2 genome
12 hours of processing time (up to 3072 samples on NovaSeq or 384 samples on NextSeq instruments)
Nasopharyngeal, oropharyngeal and nasal swabs
FDA's list of serological assays that should not be distributed [8]
U.S. FDA recommends health care providers to "be aware that not all marketed serological tests have been evaluated by the FDA"[8]
53 EUA serological assays have been removed from the FDA website notification list and should no longer be used for COVID-19 testing [30]
An independent study conducted by a federally funded national laboratory has found that 15 of 20 commercial SARS-CoV-2 antibody assays should not be marketed [8,31]
Study assays were each compared against 110 frozen serum samples with known IgM and IgG status (30 positive and 80 negative)
Performance characteristics were evaluated, including sensitivity, specificity, positive predictive value and negative predictive value (assumed prevalence of 5%)
EUA authorization was granted for 5 serological assays based on this study:
Biohit Healthcare (Hefei) Co., Ltd. SARS-CoV-2 IgM/IgG Antibody Test Kit
Euroimmun SARS-COV-2 ELISA (IgG)
Hangzhou Biotest Biotech, Co., Ltd. Covid-19 IgG/IgM Rapid Test Cassette
Hangzhou Laihe Biotech Co., Ltd. Novel Coronavirus (2019-nCoV) IgM/IgG Antibody Combo Test Kit (Colloidal Gold)
Healgen COVID-19 IgG/IgM Rapid Test Cassette
15 serological test kit manufacturers received “should not be distributed” status or market withdrawal notice based on unacceptable assay performance:
Abacus Pharma International; Accudiagnostics; Atlas-Link (Beijing); Aurora Biomed Inc.; Biomedomics; ChemBio; Chemtron Biotech, Inc.; GP Getein Biotech, Inc.; Phamatech; SD BIOSENSOR, Inc.; Shanghai Fosun Long March Medical Science Co., Ltd.; TESTSEALABS; Tianjin Beroni Biotechnology Co., Ltd.; W.H.P.M, Inc.; Zhongshan Bio-Tech Co LTD
(B) Miscellaneous Narrations And Discussions From Some Case Reports, Case Series And Studies Related To COVID-19 Infection And The Urinary Bladder As Well As Lower Urinary Tract Symptoms (LUTs)
Lamb et al. [32] made the ensuing iterations related to COVID-19 infection:
Coronavirus disease 2019 (COVID-19) does cause a wide range of symptoms that include many unexpected symptoms including a loss of taste, skin changes, and eye problems.
They had recently found patients who had documented COVID-19 infection who had developed new-onset severe genitourinary symptoms, most notably urinary frequency of equal to or more than 13 episodes voiding in 24 hours and nocturia of equal to or more than 4 episodes of voiding per night.
They had called these associated urinary symptoms COVID-19 associate cystitis (CAC).
COVID-19 severity is associated with inflammation.
They had collected urine samples from COVID-19 patients that included patients had CAC, and they had found elevation of proinflammatory cytokines also within the urine.
It had been previously demonstrated that patients who have urinary incontinence and ulcerative interstitial cystitis/bladder pain syndrome had elevated urinary inflammatory cytokines in comparison with normal controls.
There therefore postulated that CAC, with manifestation of de novo severe urinary symptoms, could occur in COVID-19 and it is caused by increased inflammatory cytokines which are released into the urine and/or expressed within the urinary bladder.
The most important implications of their hypothesis include: (a) Physician who are caring for COVID-19 patients should be aware of COVID-19 associate cystitis (CAC); (b) De novo urinary symptoms should be included in the symptom complex that is associated with COVID-19; and (c) COVID-19 inflammation may emanate in urinary bladder dysfunction.
Welk et al. [33] stated that early reports had indicated that coronavirus disease 2019 (COVID-19) could manifest with significant urinary frequency and nocturia, and that these symptoms do correlate with markers of inflammation within the urine. Welk et al. [33] evaluated surrogate markers of chronic urinary symptoms to determine if they were more frequent after COVID-19 infection. With regard to the methods, Welk et al. [33] stated that they had routinely collected data from the province of Ontario which they utilized to undertake a matched, retrospective cohort study. They identified patients who were 66 years of age or older who had a positive COVID-19 test between February 2020 and May 2020 and who had survived at least 2 months after their diagnosis. Welk et al. [33] matched them to two similar patients who did not have a positive COVID-19 test during the same time period. Welk et al. [33] measured the frequency of urology consultation, cystoscopy, and new prescriptions for overactive bladder medications during a subsequent 3-month period. Welk et al. [33] adjusted proportional hazard models for any baseline differences between the groups. Welk et al. [33] summarized the results as follows:
They matched 5617 patients who had COVID-19 to 11,225 people who did not have COVID-19.
The groups were similar, apart from a higher proportion of patients having hypertension and diabetes within the CoVID-19 cohort.
There was no significantly increased hazard of new receipt of overactive bladder medication (hazards ratio [HR]: 1.04, p = 0.88), urology consultation (HR: 1.40, p = 0.10), or cystoscopy (HR: 1.14, p = 0.50) among patients who had COVID-19, in comparison with the matched cohort.
Welk et al. [33] concluded that surrogate markers of potential bladder dysfunction were not significantly increased in the 2-5 months after COVID-19 infection.
Dhar et al. [34] stated the following:
Clinical symptoms that are manifested early in coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), had been previously well-reported.
It has been stated that even though the majority number of patients who have COVID-19 infection, do develop mild symptoms and a small percentage of the patients could progressively develop acute respiratory distress syndrome and multiple organ dysfunction syndrome resulting in death [35]
It has been iterated that there is an emergence of new symptoms which do involve many organ systems, some more subtle in comparison with others. As these symptoms could overlap with other common disease processes, it had been difficult to identify and link these symptoms as direct association with COVID-19 as the underlying cause [36]
Mumm et al. [37] not long ago had reported increased urinary frequency in COVID-19 patients.
They noticed within their tertiary care medical centre’s COVID-19 clinic that patients had reported new onset urinary tract symptoms and therefore they did obtain institutional review board (IRB) approval for a case series.
They had surveyed urinary symptoms in patients who were followed-up in the outpatient setting after their hospitalization from COVID-19.
All of patients had confirmed positive SARS-CoV-2 molecular diagnostic test.
The patients had filled out their survey responses in the office setting.
Urinary symptoms were based upon a validated bladder health questionnaire (Overactive Bladder (OAB) Assessment Tool) [38]
The five individual symptom scores ranged from 0 to 5 based upon urinary urgency, urge incontinence, incontinence, frequency, and nocturia.
They had noted the patient’s hospital dates to establish the length-of-stay (LOS) and the study was conducted from May 22 to June 26, 2020.
They had identified 39 COVID-19-positive patients that included seven females and 32 males, who had developed new-onset urinary symptoms without urinary tract infection per standard urine culture and sensitivity testing.
The patients were all outpatients following their hospital discharge and they did not have fever or other clinical conditions that would require inpatient health care.
All of the patients were African American.
The Median LOS was 10 days (range 5 - 30).
All 39 patients had completed the symptom score survey.
The median total OAB symptom score in men and women was 18 (ranges 12 - 20 and 15 - 21, respectively)
Their case series did bring awareness to the possibility of the development of new onset urinary symptoms in COVID-19 patients and the cause of the symptoms had remained unsolved.
The most remarkable urological complaints included increased urinary frequency of equal to or more than 13 voiding episodes in 24 hours in 85% of the cases and nocturia of equal to or more than four voiding episodes per night in 87% of the cases.
Dhar et al. [34] made the following conclusions: m
In a limited survey of patients within a tertiary care COVID-19 clinic, they had found that COVID-19 patients, both men and women, could report de novo lower urinary tract symptoms.
The most bothersome new urinary tract symptoms included urinary frequency and nocturia.
Physicians who care for COVID-19 patients should be aware of COVID-19-associated cystitis (CAC).
Can et al. [39] stated the following:
The COVID-19 pandemic was the most important public health problem in 2020.
Millions of people had been infected or died because of the outbreak of COVID-19
The common symptoms of the disease that they knew included fever and cough. Nevertheless, all the symptoms and features of COVID-19 were still not known.
They had aimed to evaluate the change in lower urinary tract symptoms (LUTS) after COVID-19 in men.
Can et al. [39] stated that with regard to the method of their study, they had prospectively assessed 94 patients who had COVID-19 during hospitalisation. The patients were divided into two groups according to age, that being over and under age 50. IPSS scores of all patients were enrolled. Furthermore, they compared the scores with pre-COVID-19 values. Can et al. [39] summarized the results as follows:
They assessed a total of 94 participants. The number of patients within the under age 50 group was 32 and in the over 50 age group was 62.
The mean age of all patients was 57.5 ± 16.6 years and mean body mass index was 26.2 ± 4.1 kg/m2.
Within the under 50 age group, the IPSS score before COVID-19 was 1.3 ± 1.6 and during COVID-19 it was 1.5 ± 1.6. There was no statistically significant change in the scores (P = .053).
Within the over 50 age group, the IPSS score before COVID-19 was 5.1 ± 4.1 and during COVID-19 it was 9 ± 6.4. The IPSS score during COVID-19 was statistically significantly higher than the previous score (P < .0001).
Based upon the correlation analysis, there was no correlation between IPSS scores and CT scores of all patients (P = .485).
Can et al. [39] made the following conclusions:
It had been nearly 8 months since the pandemic was announced and they could be still at the early phase of the outbreak.
All features of COVID-19 were still uncertain.
It is important to identify patients who have subclinical or non-specific symptoms to prevent or slow the spreading of the virus.
Urinary irritative symptoms could occur regardless of COVID-19 severity.
Lower urinary tract symptoms (LUTS) could be one of the symptoms of COVID-19 in some patients. Elderly patients with increased LUTS should be evaluated for COVID-19 when the reason unclear.
Nevertheless, prospective large studies are necessary to validate their findings.
Kaya et al. [40] undertook a study to show if lower urinary tract symptoms (LUTS) could be symptoms of COVID-19 with validated questionnaires. With regard to methods Kaya et al. [40] stated that the 96 COVID-19 patients who were hospitalised within a tertiary centre were collected retrospectively. After the exclusion criteria, 46 patients had constituted the study population. All of the patients then filled the forms related to the International Prostate Symptom Score and Urinary Symptom Profile respectively. All patients responded to these questions for the three period. Kaya et al. [40] summarized the results as follows:
Twenty-seven female that amounted to 58.6% of the cases and 19 male that amounted to 41.4% of the COVID-19 patients answered the questions.
With regard to the male patients, while there were no statistically significant differences in the total IPSS, the voiding IPSS score, and quality of life between the three periods (P = .148; P = .933, P = .079, respectively), the storage IPSS scores had a significant difference between the three periods (P = .05).
With regard to the female patients, low stream scores were similar between the three periods (P = .368). The scores of stress incontinence and an overactive bladder had a significant difference between the three periods (P = .05 and P = .05).
Kaya et al. [40] concluded that lower urinary tract symptoms (LUTS), especially storage urinary symptoms, could be one of the initial manifestations of COVID-19 and therefore clinicians should evaluate lower urinary tract symptoms (LUTS) with other known symptoms of the COVID-19 virus when a patient is suspected of having COVID-19 infection.
Kashi et al. [41] investigated the literature on the presence of COVID-19 virus in urine of infected patients and they evaluated the attributes and clinical significance of COVID-19 in urine including probability of infection transmission through urine. Kashi et al. [41] undertook a systematic review of literature from December 2019 to 6th May 2020 based upon data they had obtained from various data search bases including PUBMED, google scholar, OVID, Scopus and ISI web of science. With regard to eligibility criteria, they included Studies which had investigated urinary viral shedding of COVID-19 in infected patients. With regard to the study appraisal and synthesis methods, two reviewers selected relative studies and performed quality assessment of individual studies. Meta-analysis was performed on the pooled case reports and case series. Fixed-effects model was utilized for analysis as no significant heterogeneity was observed between studies. Kashi et al. [41] summarized the results as follows:
Thirty three studies were finally included in the systematic review which included 12 case reports, 20 case series, and one cohort.
Urinary samples from 430 patients were investigated.
Ten of the studies had reported the presence of COVID-19 in urinary samples from 16 patients.
The rate of presence of COVID-19 within the urinary samples was 3.7%.
Urinary viral load was low in most of the reports.
The presence of virus within urine was not related to the disease course of the illness.
Urinary COVID-19 was most often detected from patients who had moderate to severe disease which was found in 13 patients; but was also isolated from two children that included one neonate and one 7 year-old girl and one adult with mild disease.
The pathogenicity of virus isolated from urine had been demonstrated in cell culture media in one study.
Kashi et al. [41] made the ensuing concluding iterations:
Their review had highlighted the low frequency of COVID-19 presence in urine of infected individuals and the potential of isolated virus for cytopathic effects.
Therefore the probability of transmission of infection through urine could be suggested.
Caution should be exerted in dealing with urine of patients who are infected with COVID-19 including medical interventions like endoscopy and urethral catheterization
Mumm et al. [37] stated that the current coronavirus disease 2019 (COVID-19) pandemic does pose a challenge for physicians with regard to triaging patients in the emergency rooms. Mumm et al. [37] found a potentially dangerous overlap of classical urinary symptoms and the as yet not fully described symptoms of COVID-19. They reported a patient who was primarily triaged as a urosepsis case and then subsequently diagnosed with COVID-19, and based upon this experience they focused on an increase in urinary frequency as a symptom of COVID-19 and identified this in seven males out of 57 patients currently being treated within their COVID-19 wards. The details of their case is as follows:
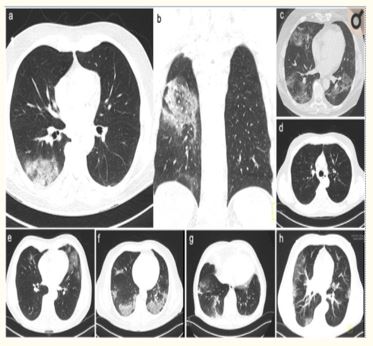
Mumm et al. [37] reported a case of a patient with suspected urinary sepsis who was admitted to the emergency department of a university hospital. The patient had reported symptoms of fever, shivering, flank pain, urgency, as well as increased urinary frequency as initial symptoms. The initial urine analysis of the urine sediment and urine culture did not reveal any signs of infection. The patient was discharged home with oral antibiotics. As part of the routine work-up assessment within German hospitals, a nasopharyngeal swab which had been taken on the same day did revealed a positive result for SARS-CoV-2 based upon polymerase chain reaction (PCR) the following day. The patient was subsequently re-admitted to one of the specialized COVID-19 wards of the university hospital in view of aggravating symptoms that included fever, fatigue, and breath-dependent chest pain. Mumm et al. [37] considered the fact that urinary frequency is a common symptom that tends to be associated with urinary infection. In order to ascertain if urinary tract symptoms were in other patients who had COVID-19, Mumm et al. [37] retrospectively and prospectively looked at patient histories for the presence of urinary frequency upon admission to their specialized COVID-19 wards. Within the time period from 16th March 2020 to 13th April 2020, seven males out of 57 patients had reported an increase in their urinary frequency contemporaneously with dry cough with regard to 5 patients, fever in 3 cases), and shortness of breath in 3 cases as leading symptoms. All of the patients had tested positive for SARS-CoV-2 within their nasopharyngeal swabs and they had developed pulmonary symptoms which were detectable based upon radiology imaging (see figure 1). Assessment of the micturition protocol did reveal an average of 13.7 urinations episodes per day on the day of admission and 11.6 on the 5th day of admission. With regard to all the patients, urinary infection, acute renal injury, and prostatitis had been excluded based upon the results of their urine analysis and normal serum creatinine and prostate-specific antigen (PSA), respectively. Prostate volumes were ascertained by means of ultrasound scanning, which had demonstrated mildly enlarged prostate gland in all of the patients; and there were no signs of residual urine or significant thickening of the wall of the bladder. SARS-CoV-2 RNA was not detected by PCR in any urinary specimens taken from all the patients during the first week after admission. Two of the patients had detectable SARS-CoV-2 RNA within serum during this period (Ct value 40). None of the patients had needed to be admitted into the intensive care unit. The average length of stay was 15 days. Mumm et al. [37] stated that the reason for the development of higher urinary frequency had not been clarified so far, as the patients did not have any signs of acute kidney injury, bacterial infection, or prostatitis. Mumm et al. [37] were of the opinion that viral cystitis due to SARS-CoV-2 causes the urinary frequency symptom. Mumm et al. [37] additionally stated that it is not clear whether replication of SARS-CoV-2 RNA in urothelial cells or secondary effect[s due to local or systemic inflammation, such as endotheliitis [42] https://pubmed.ncbi.nlm.nih.gov/32325026/], are a hallmark in COVID-19 patients which lead to symptoms such as irritative symptoms of the lower urinary tract and high urinary frequency. Mumm et al. [37] also reported that interestingly, three of the patients had presented with non-visible haematuria, which would possibly further support the postulation of SARS-CoV-2–induced viral cystitis upon infection of urothelial cells. Mumm on the other hand, iterated that they did not identify viral RNA within the urine of these patients, so it would appear that urine is unlikely to be a potential source of infection, at least in within their cohort of patients. With regard to the clinical implications of their reported case and the result of their study Mumm et al. [37] made the ensuing summations:
Classical symptoms of urinary tract infection or urosepsis such as fever and frequent urination could be misleading during the current COVID-19 pandemic.
On the whole, the diagnosis of COVID-19 has been stated to be challenging in view of the fact that patients often manifest with unclear or even subclinical signs of disease [43]
Contaminated urine samples could hamper an accurate interpretation of urine diagnostics.
Additionally, urology patients often tend to have ureteric stents or other prosthetic devices which could lead to infected sediments in analysis of urine.
Considering that these patients often tend to be elderly or immunocompromised as well as they also tend to have comorbidities such as cancer or diabetes, they do represent a high-risk cohort of patients for the development of both urosepsis and severe COVID-19 disease.
It is therefore their opinion that in the current COVID-19 pandemic, laboratory work-up of patients who have lower urinary tract symptoms should include blood tests such as full blood count, interleukin-6, ferritin, procalcitonin, serum PSA (in males), and C-reactive protein, as well as urinary examination (microscopy and culture) and nasopharyngeal swab testing for SARS-CoV-2 RNA.
These diagnostic tools could be critical with regard to the differentiation between COVID-19 and urological diagnoses in patients who manifest with urinary frequency.
Mumm et al. [37] made the ensuing conclusions:
They had identified higher urinary frequency as an additional symptom of SARS-CoV-2 infection which is independent of acute renal injury or urinary tract infection in a small series of hospitalized patients.
In view of the fact that urinary frequency along with clinical symptoms and signs including fever and positive laboratory results for inflammatory markers could be misinterpreted as urosepsis, knowledge of this finding should be important for urologists during the current COVID-19 pandemic.
In the absence of any other causes, urinary frequency may be secondary to viral cystitis due to underlying COVID-19 disease.
They would propose that clinicians should consider urinary frequency as an anamnestic tool in patients with infective symptoms in order to increase awareness among urologists during the current COVID-19 pandemic so as to prevent fatal implications of misinterpreting urological symptoms.
Additional research is necessary in order to understand the molecular mechanisms that emanate into urinary frequency that is potentially attributed to viral cystitis in SARS-CoV-2–infected patients, and to ascertain its prognostic value.
Since January 2020 Elsevier has created a COVID-19 resource centre with free information in English and Mandarin on the novel coronavirus COVID-19. The COVID-19 resource centre is hosted on Elsevier Connect, the company's public news and information website. Elsevier hereby grants permission to make all its COVID-19-related research that is available on the COVID-19 resource centre - including this research content - immediately available in PubMed Central and other publicly funded repositories, such as the WHO COVID database with rights for unrestricted research re-use and analyses in any form or by any means with acknowledgement of the original source. These permissions are granted for free by Elsevier for as long as the COVID-19 resource centre remains active.
Karabulut et al. [44] investigated the effectiveness of benign prostatic hyperplasia (BPH)-related lower urinary tract symptoms (LUTS), which does occur as a natural result of aging process and exposure to androgen, with regard to the prediction of the prognosis of disease in males who are diagnosed as having COVID-19 infection. They undertook a planned prospective study which included 63 male patients who were older than 40 years of age and who were diagnosed as having COVID-19, based upon positive results of reverse transcription polymerase chain reaction tests (PCRTs) of oropharyngeal and nasopharyngeal swabs that were obtained as per the World Health Organization guidelines. The presence of lower urinary tract symptoms (LUTS) was assessed based upon the International Prostate Symptom Score (I-PSS), a subjective assessment, and the I-PSS was filled for the patients who were included in the study. The patients were divided into three different groups based upon their scores in the I-PSS survey as follows: group 1: mild (with scores of 0 to 7), group 2 moderate (with scores of 8 to 19), group 3 severe (with scores of 20 to 35). Karabulut et al. [44] statistically analysed the data of all of the three groups. Karabulut et al. [44]] reported that with regard to the assessment that was undertaken between the groups, it was found that with regard to the patients in group 3, their length of hospital stay was longer, intensive-care requirement was more frequent, as well as their mortality rates were numerically higher. With regard to the evaluation that was undertaken on the time to admission into the intensive care unit, this was found to be the shortest in group 3. Karabulut et al. [44] concluded that based upon the results of their study, it was their opinion that in patients with COVID-19, benign prostatic hyperplasia (BPH) - related lower urinary tract symptoms (LUTS) could guide clinicians to predict the prognosis of the patients.
Creta et al. [45] searched various internet data bases to find studies that had been published up to December 2020 related to the involvement of the urinary bladder as well as the male genital systems by COVID-19. Creta et al. [] identified sixteen studies which had involved 575 patients that included 538 males and 37 females and these individuals were included in their systematic review. Creta et al. [45] summarized the results as follows:
They found that the COVID-19 phase was available for 479 of the patients and 426 of the patients were in the acute phase of the disease and 53 patients were in the recovery phase of the disease.
New-onset lower urinary tract symptoms (LUTS) were identified in 43 of the patients as well as deterioration of pre-existing lower urinary tract symptoms (LUTS) was found in 7 of the patients.
Haematuria related to bleeding from the urinary bladder was found in three patients and acute retention of urine was found in one patient.
With regard to the male genital system, they found that 8 patients had scrotal discomfort, 14 patients had scrotal swelling, 16 patients had scrotal pain, 1 patient had erythema of the scrotum and 2 patients manifested with low-flow priapism.
The undertaking of ultrasound scan did demonstrate features of: acute orchitis with regard to 10 patients, acute epididymitis with regard to 7 patients, as well as acute epididymo-rchitis with regard to 16 patients.
A case controlled study did report patients who had moderate COVID-19 infection did demonstrate a significant reduction in their sperm concentration, the total number of spermatozoa per each ejaculate, progressive motility, as well as complete mobility.
Some cases of COVID-19 infection of the urinary bladder may manifest with sudden onset of De novo lower urinary tract symptoms of urinary frequency, urgency, nocturia, urge incontinence or on rare occasion’s haematuria or retention of urine and these symptoms may or may not be associated with respiratory tract symptoms, fever, or lethargy.
Other cases of COVID-19 infection of the urinary bladder could be asymptomatic or they manifest as sudden worsening of previous lower urinary tract symptoms which may or may not be associated with fever and or respiratory tract symptoms.
The best thing every clinician can do during this COVID-19 pandemic include: to have a high index of suspicion so as to exclude the possibility of COVID-19 infection in every individual who develops new onset lower urinary tract symptoms or sudden worsening of lower urinary tract symptoms alone or with other non-specific symptoms in order to ensure all these patients undergo COVID-19 PCR tests.
Clinicians should endeavour to encourage all adults globally to have COVID-19 vaccinations.
None
Acknowledgement to European Urology, European association of Urology and Elsevier for granting permission for reproduction of contents and figures from their journal article under the Creative Commons Agreement provided the original source is credited under Copyright © 2020 European Association of Urology.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
